
Hi, help us enhance your experience
Hi, help us enhance your experience
Hi, help us enhance your experience
5438 Views
Dr Gayatri S, MD, DM, FACE, Associate professor of endocrinology and metabolism, SVIMS, Tirupati 12 June 2025
Prediabetes and CKD: A Growing Double Burden
The rising prevalence of prediabetes and chronic kidney disease (CKD) in India reflects an often-overlooked interaction in the early phases of this metabolic disease. An analysis of 19,66,449 adult HbA1c samples from India found 22.25% of the studied population to have prediabetes,[1] while pooled data from Indian community-based studies reported a CKD prevalence of 13.24%.[2] On a global scale, the International Diabetes Federation (IDF) (2025) reported 634.8 million adults (12%) with impaired glucose tolerance (IGT), with South-East Asia showing the highest burden at 13.8%.[3] Beyond overt diabetes, prediabetes and insulin resistance are increasingly recognized as contributors to early renal dysfunction. Low-grade inflammation and neurohormonal activation, the hallmarks of insulin resistance, are implicated in glomerular hyperfiltration, albuminuria, and early glomerular filtration rate (GFR) decline.[4]
Prediabetes & Correlation with CKD Onset: Evidence from the latest 2025 CURE-CKD Study
The Center for Kidney Disease Research, Education, and Hope Chronic Kidney Disease (CURE-CKD) Registry cohort study (2025) analyzed 281,933 adults with prediabetes, defined per American Diabetes Association (ADA) criteria. Over a median 2.5-year follow-up, 3.6% (n=10,104) developed CKD, with a standardized incidence of 10.9 cases per 1000 person-years. Incidence increased with age and was higher in individuals with hypertension or atherosclerotic cardiovascular disease (ASCVD) (11.9 vs. 9.4 per 1000 person-years).
Mechanistic findings suggest that glomerular hyperfiltration and high-normal albuminuria, early renal abnormalities, are more common in prediabetes. These alterations, likely driven by low-grade inflammation and hyperfiltration-induced stress, may promote CKD progression even before diabetes onset.[5]
Potential Role of Metformin in Early Renal Risk: Renal Protection Beyond Glycemic Control
In a nationwide Scottish cohort of 4,278 adults with type 2 diabetes and newly diagnosed stage 4 CKD, stopping metformin within 6 months was associated with a 26% higher risk of all-cause mortality (hazard ratio [HR] 1.26, 95% CI: 1.10–1.44).[6] A recently published 2025 cohort study analyzed 10,330 matched patients with estimated GFR (eGFR) ≥60 mL/min/1.73 m² found that metformin reduced the risk of end-stage renal disease (ESRD) by 35% and preserved renal function.[7]
The figure below presents key mechanisms by which metformin confers renoprotective effects in diabetic kidney disease.
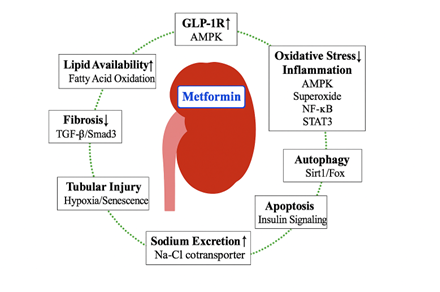
Figure: Key pathways of metformin’s renoprotective action in diabetic kidney disease (DKD), including AMP-activated protein kinase (AMPK) activation and suppression of fibrosis, inflammation, and oxidative stress. Adapted from Kawanami D, et al. Int J Mol Sci. 2020;21(12):4239. doi:10.3390/ijms21124239
TGF-β1 – Transforming Growth Factor Beta 1; Smad3 – Mothers against decapentaplegic homolog 3 (a downstream signaling protein in TGF-β pathway); NF-κB – Nuclear factor kappa-light-chain-enhancer of activated B cells, STAT3 – Signal transducer and activator of transcription 3; Sirt1 – Sirtuin 1 (a NAD⁺-dependent deacetylase involved in autophagy and stress resistance); FoxO1 – Forkhead box protein O1 (a transcription factor involved in oxidative stress resistance and autophagy); Na-Cl cotransporter – Sodium-chloride symporter, a renal tubular transporter involved in sodium reabsorption
Metformin Use in CKD: What the Guidelines Say
|
Guideline
|
Recommendations |
|
Asian Pacific Society of Nephrology (2025) |
Recommends metformin as first-line therapy in diabetic kidney disease with eGFR ≥30 mL/min/1.73 m². Dose adjustment is advised for eGFR 30–44, and discontinuation below 30. Initiation is discouraged if eGFR is <45.[8] |
|
ADA (2025) |
Advised using metformin if eGFR is ≥30 mL/min/1.73 m², with 50% dose reduction for eGFR 30–44, and discontinuation when eGFR falls below 30.[9] |
|
KDIGO (2024) |
Recommends continuing metformin in CKD patients with eGFR ≥30 mL/min/1.73 m², using lower doses if eGFR is 30–44, with individualized risk-benefit assessment.[10] |
|
ADA-KDIGO (2022) |
Consensus recommends metformin as first-line therapy in type 2 diabetes with CKD and eGFR ≥30 mL/min/1.73 m². A reduced dose (500–1000 mg daily) is advised for eGFR 30–44, and it should be discontinued if eGFR falls below 30 or during acute illness.[11] |
Key Considerations for Practice
Since metformin is now approved for use in patients with eGFR as low as 30 mL/min/1.73 m², regular eGFR monitoring is essential to guide dosing. Urine albumin-creatinine ratio (UACR) testing aids in detecting early glomerular injury and risk stratification.
Though rare, lactic acidosis risk warrants caution during acute illness or in elderly patients with declining renal reserve. To avoid therapeutic inertia, early renal risk, such as hyperfiltration or high-normal albuminuria, should prompt timely intervention in individuals with prediabetes. 8-11
Take Home Message
● A significant portion of Indian adults show early metabolic risk, with widespread prediabetes and rising chronic kidney disease prevalence.
● In the CURE-CKD study, over 10,000 individuals with prediabetes progressed to CKD within just 2.5 years.
● Metformin may offer renal protection in prediabetes through AMPK activation, anti-inflammatory, and anti-fibrotic pathways.
● Guidelines from Asian Pacific Society of Nephrology (APSN), Kidney Disease: Improving Global Outcome (KDIGO), ADA, and the ADA-KDIGO consensus recommend the consideration of metformin in CKD patients with an eGFR of≥30 mL/min/1.73 m².
References
● Vora H, et al. Prediabetes and diabetes in India: An HbA1c based epidemiology study. Diabetes Res Clin Pract. 2024;217:111889.
● Talukdar R, et al. Chronic kidney disease prevalence in india: a systematic review and meta-analysis from community-based representative evidence between 2011 to 2023. Nephrology (Carlton). 2025 Jan;30(1):e14420. doi: 10.1111/nep.14420.
● International Diabetes Federation. IDF Diabetes Atlas. 11th ed., 2025,www.diabetesatlas.org. Accessed on 3rd June 2025.
● Rico Fontalvo J, et al. Prediabetes and CKD: Does a causal relationship exist. Nefrologia (Engl Ed). 2024;44(5):628-38.
● Alicic RZ, et al. Incidence of chronic kidney disease among adults with prediabetes in the CURE-CKD registry, 2013-2020. Diabetes Obes Metab. 2025;27(6):3536-41.
● Lambourg EJ, et al; Scottish Diabetes Research Network Epidemiology Group. Stopping versus continuing metformin in patients with advanced CKD: A nationwide Scottish target trial emulation study. Am J Kidney Dis. 2025;85(2):196-204.e1.
● Lin YL, et al. Role of metformin in preventing new-onset chronic kidney disease in patients with type 2 diabetes mellitus. Pharmaceuticals (Basel). 2025;18(1):95.
● Liew A, et al. Executive Summary of the Asian Pacific Society of Nephrology Clinical Practice Guideline on Diabetic Kidney Disease-2025 Update. Nephrology (Carlton). 2025;30(5):e70031.
● American Diabetes Association Professional Practice Committee; 11. Chronic Kidney Disease and Risk Management: Standards of Care in Diabetes—2025. Diabetes Care. 2025;48 (Suppl_1): S239–S251.
● Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2024 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. 2024;105(4S):S117-S314
● de Boer IH, et al. Diabetes management in chronic kidney disease: A Consensus Report by the American Diabetes Association (ADA) and Kidney Disease: Improving Global Outcomes (KDIGO). Diabetes Care. 2022;45(12):3075-90.
{{Article_Title}}
{{Article_Author}}
{{Article_Title}}
{{Article_Author}}
